")
In a tethered spinal cord, the spinal cord is attached in the spinal canal and is unable to move freely in the spinal canal. A lot of causes are behind the tethered spinal cord. Several treatment options are available to treat this. Surgery is one of the options to manage it.
First of all, the patient must be diagnosed properly to decide if surgery is the right decision. The cause of the tethered cord syndrome (TCS) is evaluated because surgery is performed according to the cause of TCS. Surgery is more beneficial in early stages of life because damage of spinal nerves due to TCS is usually less in early stages of life. As the birth defect progresses the damage of spinal nerves increases. If left untreated, permanent or irreversible damage occurs. When damage is irreversible then there is no benefit of surgery as surgical intervention also has complications.
First of all, the patient is prepared for surgery. During preparation, all baseline investigations are performed to identify any problem related to other systems. Checking of vitals depends upon the age of the patient. If the age of a patient is less than 13 years, pulse rate and respiratory are more important according to the anesthesia point of view while blood pressure is important in the patients with an age greater than 13. The respiratory system and central venous system is assessed thoroughly. General anesthesia (GA) is best for tethered spinal cord surgery. Anesthesia is designed to make the patient pain free. In GA, whole body is made pain free.
After assessing the patient and declaring him/her fit for anesthesia, the patient is brought to the operation theatre (OT). In OT, the patient is laid on the OT table. The injection of anesthesia is given through IV cannula to make the patient unconscious with the effect of anesthetic injection. An endotracheal tube (ETT) is passed into the trachea (the tube which connects mouth to the lungs and helps in respiration) quickly. An oxygen mask is attached to the ETT for the artificial supply of oxygen to lungs. After doing all of this the main surgery is started.
The patient’s position is changed from supine to prone because the spinal cord is approached through back. The affected area is exposed and antiseptic measures are performed on the exposed area.
To approach the spinal cord, laminactomy is performed first. Laminactomy refers to “a small piece of bone removed from the vertebra”. To do laminactomy, an incision is made in the skin. The muscles and tissues under the skin are separated. Vertebra is exposed. A small piece of bone is removed from the vertebra. After removal of the bone the spinal canal is approached.
When an approach is made to the spinal canal, the surgeon must identify the spinal cord and spinal nerves. After identification of the location of tethered cord, the cause of TCS is identified. If any fatty tissue or mass is present, it is removed first. Any other cause is also managed accordingly. Now the attached spinal cord is just in the range of the surgeon’s vision.
The main steps of surgery start now. The spinal cord and spinal nerves are checked. As the spinal cord and nerves are very thin and small a microscope is used to identify them. A neuro-physician is present to check the motor and sensory nerve supply of lower limbs. Any deterioration in the function of spinal nerves is checked and conveyed to the operating surgeon. The spinal cord is separated from the spinal canal. Spinal nerves are also separated from each other and adjusted at their places. If any split or tear is present on the spinal cord or nerve, it is also repaired by stitching. After doing this, the spinal canal is closed by placing a patch on the protective covering of spinal cord. The patch is stitched with the covering. The patch is placed to avoid leakage of cerebrospinal fluid (CSF) through the operated site. Up till now, the main part of this surgery is completed. Bleeding is secured by diathermy, stitching or applying pressure on the bleeding vessels. The muscles and tissues underlying the skin are approximated. The skin is stitched with fine sutures to minimize the scar mark. Antiseptic measures are applied on to the operated site and the dressing is placed on it.
After completing all this, the patient is assessed from the anesthesia point of view. An injection is given through IV cannula to minimize the effect of anesthesia drugs. When the patient starts to respond to a painful stimulus, ETT is removed and the patient is allowed to do spontaneous breathing. The oxygen mask is placed on the mouth to maintain the oxygen saturation until the patient starts spontaneous breathing. Again a painful stimulus is applied to check the response of the patient. When the patient is responding well and doing spontaneous breathing, he/she is considered out of anesthesia. Now the patient can be shifted to recovery room.
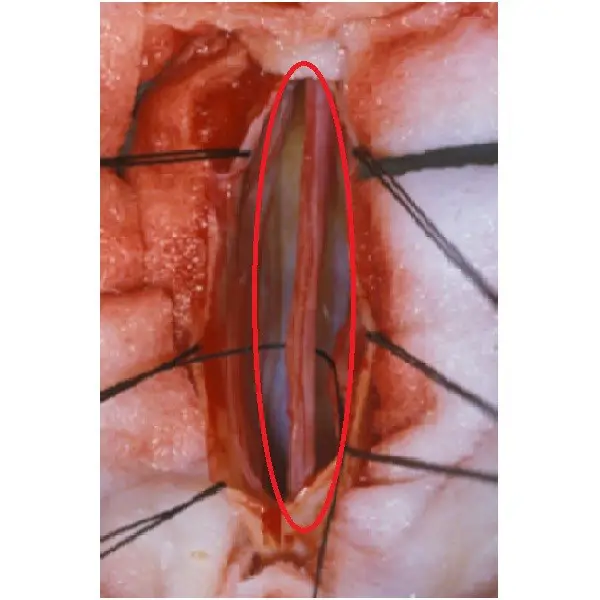
Figure 1: In this picture the spinal cord is shown. Duramater (the protective covering of spinal cord) is opened to approach the spinal cord. The location where the tethered cord is present is identified and detethered by placing a stitch behind the spinal cord. The red circle is made around the area where spinal cord is exposed by retracting the duramater (Source: www.ispn.guide.com).

Figure 2: This is a schematic diagram of the back of the patient near the lumbosacral region. This diagram shows how the approach is made through the skin to the spinal canal. A red circle is made around the incision that is made on the skin to approach the spinal canal to perform detethering of the tethered spinal cord (Source: www.ispn.guide).

Figure 3: This is the picture of a patient to whom tethered spinal cord surgery was performed. A red circle is made on the scar mark that is made on the back of patient after the healing of wound that was made on the skin in lumbosacral region to approach spinal canal (Source: www.pinterest.com)
References
1. Falci SP, Lammertse DP, Best L, Starnes CA, Prenger EC, Stavros AT, et al. Surgical treatment of posttraumatic cystic and tethered spinal cords. J Spinal Cord Med 1999;22(3):173-81.
2. Hüttmann S, Krauss J, Collmann H, Sörensen N, Roosen K. Surgical management of tethered spinal cord in adults: report of 54 cases. J Neurosurg 2001;95(2 Suppl):173-8.
We will add your organization!

